





| Is this application for a new or a repeat module | |
| New module | Repeat module |
Proposed title for the Module
Abstract (Max 250 words)
Health inequalities emerge in the intersection between social structures, individual actions and biological processes. While disease and premature mortality ultimately are biological phenomena taking place in individual bodies, social inequalities in ill health, disease and mortality are caused by socially determined conditions. There has been a strong renewed interest in health inequalities both among policymakers and in academia, even before the COVID-19 crisis From 2018, WHO organization-wide commitment to acting on health inequalities was presented in the 13th General Programme of Work 2019-2023. A new Department devoted to Social determinants of Health was also launched. The key element in this proposed second module wave is health and its broader social determinants. The European region is committed to lead the renewed effort to inform the debate on health inequalities, which was highlighted by WHO-Europe in the “Healthy, prosperous lives for all: European Health Equity Status Report” (WHO 2019). Despite the immense value of this report, it also highlighted the need for better data materials with high-quality indicators on several determinants of health. A repeat module on socioeconomic inequalities in health and their determinants will enable trend analyses and longitudinal application of the comprehensive pan-European comparative data set developed as part of the first module. The data will e.g., be used to evaluate the potency of differing European policy regimes, to track the medium-term impact of the covid-19 pandemic, and to further advance theories of social inequalities in health.
Principal Applicant
| Name | Terje Andreas Eikemo | |
| Positions | Professor of Sociology
Leader of the Centre for Global Health Inequalities Research (CHAIN) Editor-in-Chief, Scandinavian Journal of Public Health |
|
| Institution (including name of University School or Department) | Norwegian University of Science and Technology (NTNU) Department of Sociology and Political Science | |
| Address for correspondence | Building 10, CHAIN, Dragvoll, Edvard Bulls veg 1, 7491 Trondheim, Norway | |
| Telephone: +47 99034077 | Email: terje.eikemo@ntnu.no | |
ESS Round 11
Question Module Design Template
Module Title: Social inequalities in health and their determinants
Module Authors: Terje Andreas Eikemo, Mirza Balaj, Tim Huijts, Kristian Heggebø and Clare Bambra
Rationale
Our previous rotating ESS module on health and their social determinants (hereafter referred to as the Health Module), which was included in the seventh round of the ESS (2014), represented a major step forward for cross-national comparisons of social inequalities in health. The module has solved methodological challenges within sociological health research, provided new explanations of the prevalence and social distribution of poor/good health, and formed the basis for new theoretical perspectives. The module has also been widely used not only academically, but also in national and international policy-settings.
Since the first Health Module was implemented, we have seen several worrying developments of relevance for health and its social distribution.
First and most importantly, the coronavirus disease (COVID-19), which has been characterized as a pandemic by the World Health Organization (WHO), is attacking societies at their core. Measures to control COVID-19 have already put to test not only the European healthcare system, but also its economy, welfare systems, and societal trust. Moreover, scenario-based studies are predicting that the most effective COVID-19 strategy to limit the number of infections and deaths would need to be a combination of cyclic lockdown and relaxation measures over the next 18 months (1). The prolonged control measures will constitute an unprecedented challenge with very severe socio-economic consequences likely to persist long beyond the acute health crises we are currently facing (2). This pandemic has meant that public health and health inequalities are now a top research, political and public policy priority across Europe (3). It is therefore essential to collect data to monitor and compare how the burden of these negative consequences is distributed in European countries with differing policy regimes, and to what extent European policymakers are able to protect the health and wellbeing of the most vulnerable groups. A repeated Health Module provides a unique opportunity to examine the medium-term effect of COVID-19 on social determinants of health, and e.g., track developments in mental and physical health by socio- economic status and/or gender.
Second, we have observed increasing inequalities in income and wealth in many European countries (4). A repeated Health Module would e.g., allow us to examine the health consequences of increasing poverty rates. Poverty reduces financial access to activities and products that are important for the maintenance and promotion of health, such as a healthy diet, exercise, and social contacts (5). Poverty also reduces access to health care services, particularly when out-of-pocket payments are required. Moreover, poverty often leads to psychosocial stress, which increases the likelihood of risk-taking behaviors such as smoking and excessive alcohol consumption (6). Larger differences between ‘the haves’ and ‘the have-nots’ could therefore lead to an acceleration of health deterioration among vulnerable groups, which, if not timely addressed, might be further exacerbated by the COVID-19 crisis.
Third, precarious labor market attachments have grown noticeably in several European countries. Examples include temporary employment, part time and on-call work, zero-hour contracts, agency work, and ‘bogus’ self-employment (7–9). Whether, and to what extent, the increase in such insecure employment relationships is followed by more self-reported health problems (e.g., mental wellbeing, back/neck pain, blood pressure, etc.) is an important knowledge gap. Again, the ongoing pandemic may have exacerbated some of the problems associated with precarious employment and poor working conditions. Temporary contract workers are for example more likely to be placed at higher COVID-19 exposure risk through their employment and will likely be more hardly hit by the expected economic recession since people in temporary positions are more easily laid off. Furthermore, the availability and generousness of sickness benefit schemes is probably a very important mediator, calling for cross-national comparative research.
Fourth, the impact of educational expansion, i.e., higher average educational qualifications in younger cohorts, continues to be felt throughout Europe (10). Although rising levels of education clearly has many positive features, there are some unanticipated consequences as well, such as more labor market exclusion among people with few formal educational qualifications (11) (12). These individuals could be trapped in vicious circles leading to an ever more marginalized social and economic position, with possible negative effects on health. Yet, European countries differs non-negligibly in how successful they are in incorporating low educated on the labor market, again calling for comparative studies. There are fears, though, that the economic consequences of the pandemic may lead to a ‘lost generation’ of young people with low education who have a particularly high risk of prolonged unemployment (and possibly permanent labor market withdrawal), accompanied by well-established negative health effects (13).
Fifth, recent evidence suggests worrying trends in several non-communicable diseases (NCDs) with e.g., prevalence of diabetes and obesity increasing noticeably since 2014 (14–16). NCDs have major economic consequences that affect individuals, healthcare systems and societies in Europe. NCDs lead to a higher overall burden of disease in advanced capitalist societies, and to a major economic burden (i.e., healthcare costs and productivity losses). On a more positive note, downward trends have been observed for other health outcomes and behavioral risk factors such as high blood pressure, smoking, and alcohol consumption (17,18). Nevertheless, large variation exists between European countries, with trajectories moving at different speeds and in some cases even in opposing directions (19). In addition, despite close monitoring of some NCDs and behavioral risk factors by e.g., national surveys, WHO Europe, and the European Commission, far less attention has been paid to monitoring trends in socio-economic inequalities in NCDs, and to inequalities based on a more comprehensive set of social determinants. The second round of the Health Module would address these shortcomings by providing the first possibility to examine time trends in socio-economic and social inequalities in NCDs in a large number of European countries. By expanding this knowledge-base, analyses of ESS data will, first, enhance our understanding of the causal mechanisms that underlie social inequalities in health, and second, localize policy packages and interventions that might be able to reduce health inequalities in differing country contexts.
Other important societal trends can also serve as a backdrop for empirical investigations using a follow-up module. Populist and far-right political parties have entered coalition governments in several European countries in recent years, resulting in policy measures pushed forward to reduce access to welfare benefits and health services. These measures have hit vulnerable groups, such as migrants, homeless and women, particularly hard. The COVID-19 crises run the risk of reinforcing these pre-existing nationalist dynamics (20). There is also evidence suggesting that trust in the healthcare system is on a downward spiral in Europe, with an accompanying growth in mis- and disinformation via fake or poor-quality websites and social media communities, and active spoiler groups such as the anti-vax movement (21,22). Moreover, how the COVID-19 crises will further shape trust in the healthcare system might prove to be pivotal for the future of healthcare services. WHO-Europe is particularly invested in introducing a more nuanced
understanding of trust in healthcare institutions through the second Health Module. The wider context – the political, the economic and the social preferences and concerns of Europeans – covered by the ESS survey would provide more substantiated explanations concerning trust patterns in Europe which will be of interest to policy-makers more generally, and not just the health community. According to WHO-Europe, this would allow for the development of policy responses at a level and in a manner of direct relevance to citizens. Another important area of investigation is the effect of COVID-19 on female labor force participation. Although the Great Recession actually was followed by increasing employment level among women (23), the COVID-19 crisis, and the following post-crisis period, might see a substantial reduction in female labor force participation due to, first, the severe economic impact on sectors in which they are overrepresented (e.g. retail and tourism), and second, their primary caregiver role for children and elderly people (24).
Thus, several important economic, demographic, public health and political developments have given urgency to the need for a second Health Module in 2022-2023. It should also be underscored that health inequalities – and the social determinants of health framework – have become more prominent on the WHO’s agenda. Governments in several European countries, including the European Commission EU4Health Programme, have furthermore developed plans, although of varying detail and ambition, to combat social inequalities in health. To generate solid, pan- European empirical evidence, backed up by a sound theoretical framework, is therefore more urgent than ever before, and this is exactly what a second Health Module will provide.
Overall, the first Health Hodule in 2014 had no significant weaknesses in terms of item measurements. Nevertheless, we acknowledge that the inclusion of other variables (e.g., related to trust in healthcare systems) could strengthen the module noticeably.
The ESS special COVID-19 module that will become available in round 10 does not make a new Health Module in round 11 less relevant. On the contrary, they will reinforce each other. A new ESS Health module is needed as a complement to the COVID-19 module because it will enable an examination of trends by comparing levels of health determinants and health outcomes before and after the COVID-19 crisis. Furthermore, the COVID-19 module in round 10 will only be able to capture the short-term impacts of the pandemic. The COVID-19 will also have severe health impacts that will only fully manifest themselves in the longer run. For example, people who have recovered from COVID-19 may experience long-term health problems, e.g. due to lung damage. Also, given that ESS10 only includes two general questions on self-reported health and longstanding illness, the impact of COVID-19 on specific physical and mental health problems would remain unexamined. Additionally, the increased pressure on healthcare systems has already resulted in delayed diagnoses and treatment of other health issues, which may lead to an increase of e.g. non-communicable diseases over the next few years.
Governments across Europe have implemented both containment measures to limit the spread of the virus, and support measures to mitigate the economic and financial impact of the containment measures. The mental health impact of the virus and of the policy measures will depend on how long, and in what form, the chosen measures will be in place. Importantly, there is considerable cross-national variation related to (i) the spread of COVID-19, (ii) the containment measures, and
(iii) the support measures, implying that comparative research most likely will reveal intriguing insights. The impact of COVID-19, containment measures, and support measures on physical and mental health will inevitably vary according to where people are placed in the socioeconomic ‘hierarchy’, and social inequalities in health are thus expected to increase in the years to come. As such, our module would provide a unique opportunity to directly link the impact of COVID-19 to a broad range of health outcomes across European countries, and to assess whether some countries have been able to limit the impact on social inequalities in health more than others. More specifically, a follow-up Health Module in ESS11 would enable the research community to explore the medium-term impacts and dynamics of the pandemic with regards to mental and physical
health, health care access, trust in health care systems, as well as economic, labour market and other social determinants of health. Our module would therefore significantly complement the plans for ESS10 and enable analyses of differences and similarities across Europe in the more long-term impact of the crisis (especially on physical and mental health). This would be valuable information for European policymakers in terms of planning responses to any future virus pandemics.
Theoretical/conceptual approach
Social inequalities in health continue to be a key public health problem in European countries. Not only are social inequalities in morbidity and mortality reported in many European countries but they are in fact found to be substantial in all countries with available data (25,26). Comparative approaches to inequalities in health are important for at least two reasons. First, they are central to establishing the nature of health inequalities – are such inequalities a universal phenomenon or something specific for certain stages of development or historical periods? Second, and more importantly, systematic international comparisons form the basis for one of the key questions in health inequality research, namely whether or not it is possible to organize society, or welfare states, in a way that reduces or even eradicates health inequalities. The concept of welfare state regimes has therefore been increasingly used by political scientists and health sociologists to analyze cross-national differences in population health. These studies have invariably all concluded that population health is enhanced by the relatively generous and universal welfare provision of the Social Democratic Scandinavian countries (27). Yet there is large agreement that welfare states are not immovable objects but are continuously being recalibrated (28). The new engagement of the European Commission to promote the modernization of the European Welfare States through social investment is but one of the driving forces – together with the Sustainable Development Goals – that will recalibrate the breadth and depth of social spending in Europe (29), changing also their impact on conditions of living. The various social policy responses to the COVID-19 pandemic also highlight the importance of European social security safety nets (30). Although it is widely acknowledged that welfare states are important determinants of health as they mediate the extent, and impact, of socio-economic position on health, there is an urgent need to match our knowledge on the changing nature of welfare states with comparable data on health determinants and more refined health outcomes for a large number of European countries. Earlier comparative studies have suffered from important weaknesses such as a limited number of country cases and serious comparability problems (e.g., data harmonization of poor quality). Longitudinal approaches and trend analyses are also lacking in the field due to data availability issues. A second round of the Health Module would enable us to examine stability and change over time in how European welfare states, of varying size and quality, influence health and its social determinants.
The theoretical framework underpinning the second round of the Health Module will remain largely the same, with exception of the introduction of two new additional theoretical approaches that have been developed since the design of the first Health Module – one of which emerged as a result of our first module.
Population health arises from the complex interactions of individual, environmental, material and social relations (31) The level of health experienced or attainable by an individual, community or population is a direct result of the interaction and quality of the relationship between the various biological and social determinants of health (32). Systematic differences in health exist between socio-economic groups (see Figure 1). These inequalities in health between socio-economic groups are not restricted to differences between the most privileged groups and the most disadvantaged; health inequalities exist across the entire social ladder, which is often referred to as ‘the gradient’ (33). Socio-economic inequalities in health are universal within European countries and they extend along the whole societal hierarchy: “the higher the social position, the better the health” (34) . Health inequalities are thus not “natural” or “inevitable”; they are socially distribute and socially determined.
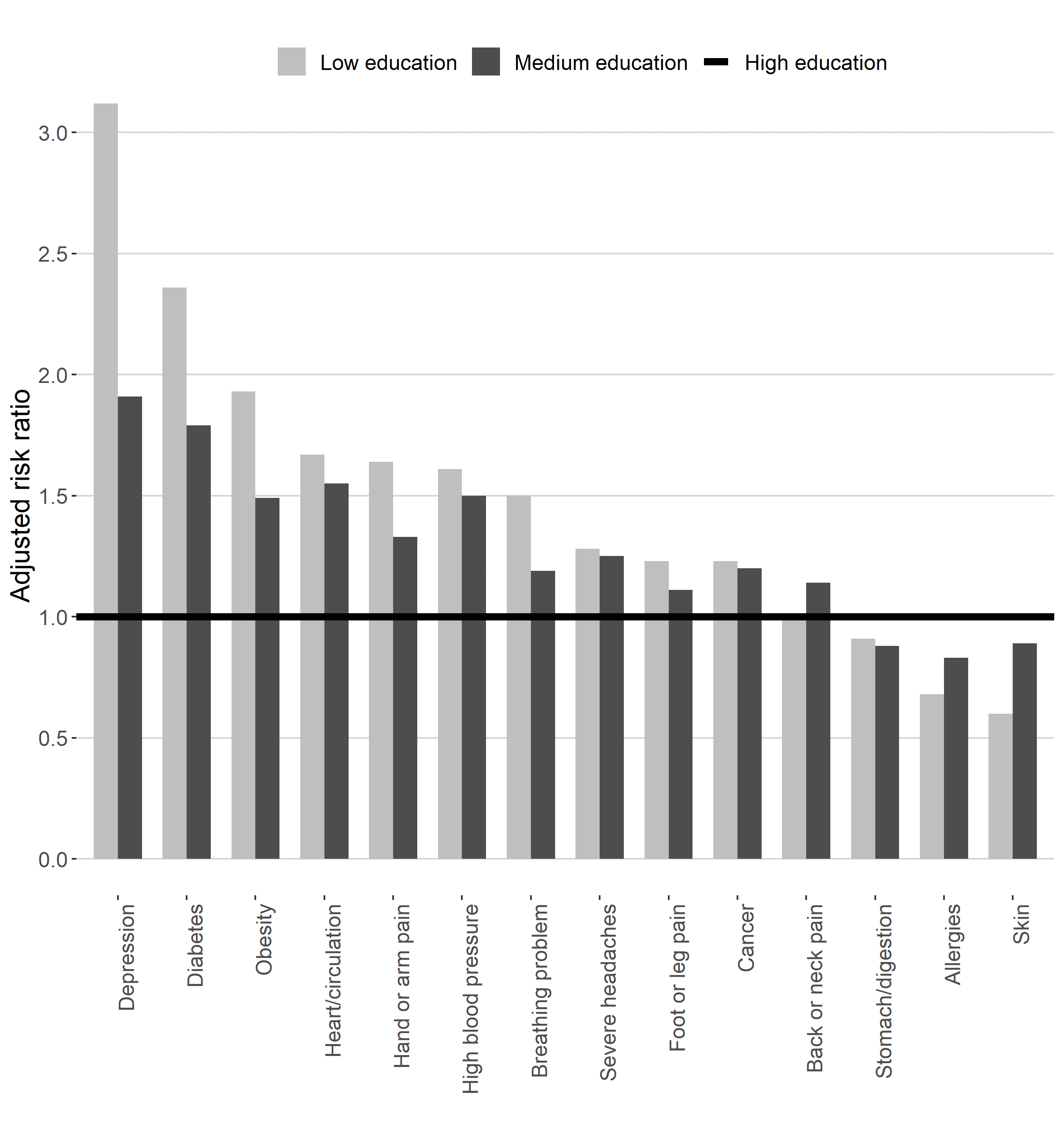

Figure 1: Educational Inequalities in Non-Communicable Diseases in Europe(26) (ESS health module 2014)
The social determinants of health are the wider cultural, psychosocial, and material conditions in which people work and live (32). These are what social epidemiologists refer to as the ‘causes of the causes’(33). The main social determinants of health are widely considered to be: access to essential goods and services (specifically water and sanitation, and food); housing and the living environment; ‘lifestyle’ factors; access to health care; unemployment and social security; working conditions; and transport (31). This is demonstrated in figure 2 (next page).
The social determinants of health are considered to influence health inequalities through various explanatory pathways. Traditionally, three main theories which attempt to explain how social determinants interact with health and inequalities in health have been used within the literature: cultural-behavioural, material and psychosocial. More recently the theory of fundamental causes has started to become more influential, as has the institutional theory of health inequalities. Members of the QDT have tested the validity of the fundamental cause theory using the Health Module (which is the first time survey data has been able to do this), and the team has also contributed to the theoretical formulation of the new institutional theory of health inequalities, which was partly based on the empirical analysis of the first ESS Health Module.
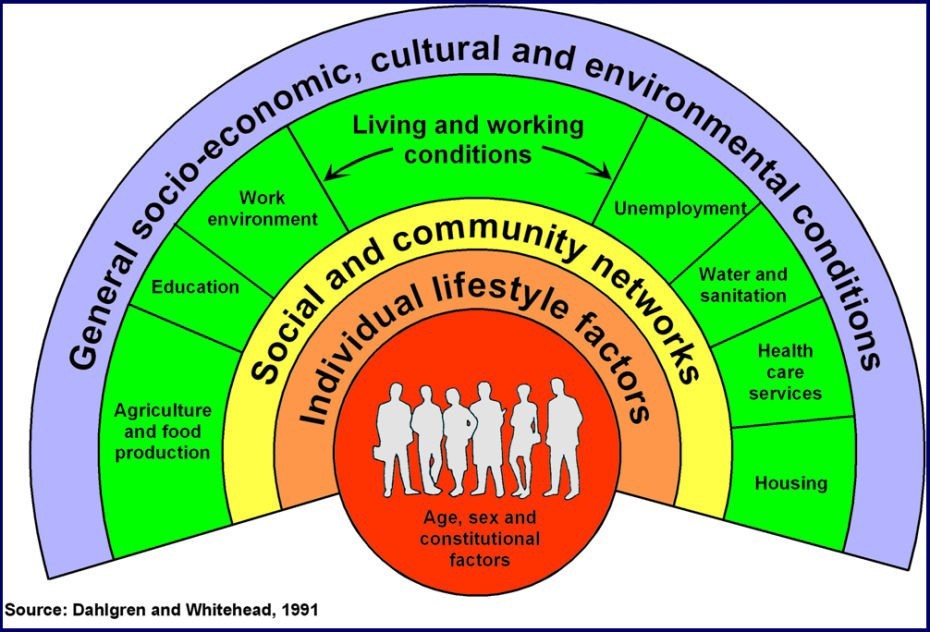

Figure 2: Dahlgren and Whitehead (1991) model of the determinants of health
Cultural-Behavioural
The cultural-behavioural approach asserts that the link between socio-economic status and health is a result of differences between socio-economic groups in terms of their health related behaviour: smoking rates, alcohol and drug consumption, dietary intake, physical activity levels, risky sexual behaviour, and health service usage. Such differences in health behaviour, it is argued, are themselves a consequence of disadvantage, and unhealthy behaviours may be more culturally acceptable amongst lower socio-economic groups. The ‘hard’ version of the cultural-behavioural approach asserts that the differences in health between socio-economic groups are wholly accounted for by differences in these unhealthy behaviours. The ‘softer’ version posits that behaviour is a contributory factor to the social gradient but not the entire explanation (35). Risky health behaviours are more concentrated amongst poorer socio-economic groups due to the concentration of individuals with less self-control, lower responsibility, poorer coping abilities, lower health knowledge, and a more short term outlook on life: an agency focused explanation which can be summed up as the ‘feckless poor’ argument. A more recent version of the behavioural model (the cultural-behavioural approach) takes into consideration the more structural role of culture and how different cultural norms can pattern the distribution of unhealthy behaviours. Unhealthy behaviours are more common in lower socio-economic groups where these behaviours represent the cultural norm and thus are more acceptable. The cultural-behavioural explanation does not take into account possible wider reasons for why unhealthy behaviours are more prevalent and/or more acceptable in lower socio-economic groups, namely the social determinants of health and other more structural factors such as the experience of deprivation and feelings of powerlessness. Simplistic behavioural explanations therefore merely lend authority to policies which stigmatize already disadvantaged individuals and communities (36). Cultural health capital is also relevant in this perspective as the further up a social hierarchy a person is located, the less exposure to health-effecting stressors (37). People with high socio-economic status will also have access to more social and psychological resources in the event of experiencing such stressors. This amounts to ‘cumulative advantage’ processes over the life course on aspects of relevance for health.
Materialist
The materialist explanation focuses on income, and the neo-materialist approach on what income enables, in the relationship between socio-economic status and health. Important dimensions of what income enables include access to goods and services and the limitation of exposures to physical, and psychosocial, risk factors. By way of illustration, a decent income enables access to health care, transport, an adequate diet, quality housing and opportunities for social participation; all of which are health promoting. Material wealth also enables people to limit their exposures to known risk factors for disease such as physical hazards at work or adverse environmental exposures. Materialist approaches give primacy to structure in their explanation of health and health inequalities, looking beyond individual level factors (agency), in favor of the role of public policy and services such as schools, transport and welfare in the social patterning of inequality (38,39). Cross-national comparisons demonstrate the importance of material factors on health and health inequalities (35). In general, countries with narrower income disparities between rich and poor have better health and wellbeing, evident for outcomes such as obesity, drug use, teenage conceptions, stress, and mental ill health (39). These countries also have better welfare services and so access to education, social housing, transport, health care provision and green spaces tend to be better and more fairly distributed across the population. This may partly account for how lower income inequality translates into better health outcomes. This evidence augments the theory that everyone does better in conditions where income inequalities are small. However, data from recent ESS studies do not suggest that relative health inequalities are smaller in more equal countries, and this represents a particular challenge for the materialist approach (40).
Psychosocial
Psychosocial explanations focus on how social inequality makes people feel and the effects of the biological consequences of these feelings on health. Bartley (2017) describes how feelings of subordination or inferiority stimulate stress responses which can have long term consequences for physical and mental health especially when they are prolonged (chronic). The socio-economic gradient is therefore explained by the unequal social distribution of psychosocial risk factors. Psychosocial risk factors associated with the workplace include low levels of control over how work is undertaken, limited autonomy over work tasks, monotonous work and time pressures, low levels of support from co-workers and supervisors, an imbalance between efforts exerted and rewards received and organizational injustice (41). Bartley (2017) underscores how it is the way stress makes people feel that is important in relation to health outcomes rather than straightforward exposures to stressors. In this way the model combines both structure and agency. For example, it may not simply be income level or an adequate working environment alone that leads to good health but rather how good income and good quality work can make people feel, especially in relation to others. Here perceptions of social status and in particular perceptions of status in comparison to other people in society are significant constructs: what matters is how individuals value themselves. If these value judgements are negative, feelings of inferiority or subordination can invoke harmful stress responses.
Fundamental causes
The discussion of the influence of the social determinants above reflects the dominant model within cross-national health research, which stems from social-epidemiological research. This model is particularly useful because it does not consider health to be primarily a product of individual action, but rather stresses the complex social determinants behind the inequalities. However, it is not fully satisfactory as a sociological model because it does not consider that the social distribution of health is also a result of how individuals actively form their own life chances and is not only the result of the social context in which individuals live. This is the core of the fundamental cause theory. Link and Phelan developed the theory of fundamental causes to explain the association between social status and mortality. They proposed that the enduring association results because social status embodies an array of resources, such as money, knowledge, prestige, power, and beneficial social connections that protect health no matter what mechanisms are relevant at any
given time (42,43). According to the authors, a fundamental social cause of health inequalities has four essential features. First, it influences multiple disease outcomes, meaning that it is not limited to only one or a few diseases or health problems. Second, it affects these disease outcomes through multiple risk factors. Third, it involves access to resources that can be used to avoid risks or to minimize the consequences of disease once it occurs. Finally, the association between a fundamental cause and health is reproduced over time via the replacement of intervening mechanisms. It is the persisting association between socio-economic status (SES) and health in the face of dramatic changes in the mechanisms linking SES and health that led Link and Phelan to call SES a “fundamental” cause of health inequalities.
Overall, through the ESS Health Module it has been possible to test and refine both the main theories (cultural-behavioral, material and psychosocial) (40,44–46) and the Fundamental cause theory (47). The richness of social determinants and health measures available in the 7th Round of the ESS has also inspired additional approaches to explain how the interaction of social determinants of health distributes health within and across societies.
Institutional theory
Recent research has turned towards the welfare state as a major explanatory factor in the search for causes of health inequality that explain the persistence and variability of health inequality across countries (27). This theory creates an organizing framework for this new scholarship by combining aspects of the materialist and psychosocial explanations with the recognition that the social determinants of health are themselves shaped by macro-level institutional and structural determinants: politics, the economy, the state, the organisation of work, and the labour market (48). Health inequalities are thus considered as politically determined by institutional (in)action (27). A wide range of research has demonstrated that even within the constraints of unequal societies, the behavioural, material and psychosocial determinants of health inequalities are themselves amenable to public policy interventions. Not all high income countries have the same levels of health inequality, and the institutional approach argues that political choices and resulting public policies are responsible for these differences (49). In doing so this theory identifies several mechanisms – redistribution, compression, mediation and imbrication – that connect the welfare state to health inequalities by producing and modifying the effects of the social determinants of health. Through applying this theoretical lens in our repeated Health module, it will be possible to better understand why we see different distributions of social determinants – and health inequalities – within European societies embedded in different welfare state traditions. The institutional approach has also highlighted the importance of how social and economic inequality intersects with race, gender and other aspects of social disadvantage (50).
An additional element of the institutional theory is whereby Bourdieu’s theory of capital is used to contextualize the experience of health across different welfare states (51). Bourdieu’s theoretical framework is particularly well suited to examine health inequalities, as capitals are equivalent to material and non-material resources relevant to individuals in the social space. When translated in the social space relative to health outcomes, these resources can be conceptualized as the resources necessary to safeguard or improve health, i.e., the social determinants of health. The main hypothesis deriving from Bourdieu’s theory is that individuals engage in constant social struggle to acquire, maintain and improve their composition and volume of social determinants of health. Integrating Bourdieu’s theory of capitals presents a new direction relative to much of the existing health inequality research, which focuses on the unidirectional causality between agency and structure (instead of understanding their relations as mutually interdependent). Social determinants of health emerge at the intersection of social practices and structures, which reflect the distribution of power and health in society. These new emerging theoretical approaches – in combination with the ‘original’ ones – can generate more comprehensive evidence, but only if we are able to map changes to the distribution of social determinants of health vis a vis institutional changes that affect various forms of capital, and how this varies across differing sociopolitical contexts.
Health inequalities due to COVID-19: the relevance of the social determinants approach
The continued importance and relevance of the social determinants of health are evident, for example, in the COVID-19 pandemic where there are stark inequalities in mortality and morbidity. There is clear evidence already of social inequalities in COVID-19 infection and mortality rates from Spain, the USA and the UK; three countries hit hard during the first phase of the pandemic. For example, intermediate data published by the Catalonian government in Spain in April 2020 suggest that the rate of COVID-19 infection is six- or seven-fold higher in the most deprived areas of the region compared to the least deprived (52). Similarly, in preliminary analysis from USA, it has been reported area-level socio-spatial gradients in confirmed cases in Illinois and New York City, with dramatically increased mortality risk observed among residents of the most disadvantaged counties (53). Official, national data in England and Wales found that COVID-19 related deaths were twice as high in the most deprived neighbourhoods (55 per 100,000 population) than in the most affluent neighbourhoods (25 per 100,000 population) (54).
The COVID-19 pandemic is occurring against a backdrop of social and economic inequalities in existing non-communicable diseases (NCDs) as well as inequalities in the social determinants of health. Inequalities in COVID-19 infection and mortality rates are therefore seen to be arising as a result of a syndemic of COVID-19, inequalities in chronic diseases, and the social determinants of health (30). People with low socio-economic status have a greater number of co-existing chronic health conditions, which are more severe and they experience the conditions from a younger age. These inequalities in chronic conditions arise as a result of inequalities in exposure to the social determinants of health (26). The social determinants of health also work to make people from marginalised communities more vulnerable to infection from COVID-19 – even when they have no underlying health conditions. Decades of research into the psychosocial determinants of health have found that the chronic stresses of material and psychological deprivation is associated with immunosuppression (55). In addition to these long-term exposures, current inequalities in working conditions may also be impacting on the unequal distribution of the COVID-19 disease burden. For example, lower paid workers are much more likely to be designated as key workers and thereby are still required to go to work and reliant on public transport for doing so. This all increases their exposure to the virus. COVID-19 is therefore being experienced as a syndemic – a co-occurring, synergistic pandemic, which interacts with existing chronic health and social conditions (Figure 3).
Figure 3: The Syndemic of Covid-19, Non-Communicable Diseases (NCDs) and the Social Determinants of Health (Bambra et al, 2020)
Implementation
The 2014 Health Module has contributed vastly to the research field of health inequalities and to policy discussions (e.g. within the European Commission and WHO Europe). Our article, which presented the module to the international audience is among the most cited studies in the European Sociological Review (56). In 2017, the health module was the most used rotating module in ESS with 30 publications (57). Although 2020 and 2021 are expected to be the peak publication years, the use of the health module has already been excellent. By 21 May 2020, 80 publications were traced, involving data from the seventh round of the ESS and particularly the integrated Health Module. Academic articles have been published in highly ranked journals in the fields of sociology, political science, medical sociology, epidemiology, public health as well as psychology, and medicine resulting in more than 1600 citations overall. This clearly demonstrates that the Health module is becoming an essential data source for researchers interested in the social determinants of health (even if the study may not deal with health at all). The Health Module is therefore of great value to researchers also outside the public health field.
The Health Module has expanded the health inequalities field through both empirical findings and theoretical development. Empirically, the first Health Module has allowed researchers to take an intersectional stance and provide ample evidence of health inequalities for various health measures based on socio-economic status (employment, occupation, education, income), gender, age, geographical location, migrant status as well as their interaction (58). Moreover, the ESS core questionnaire has been used in conjunction with the Health Module to examine health outcomes other than self-reported sealth (SRH) and activity limitation (AL), which are present in the core questionnaire. In fact, the depression scale and (multi)morbidity outcomes have been more widely used than the core questionnaire health measures (SRH/AL), which can be observed in table 1.
A series of studies using the ESS Health Module data suggest that higher levels of socio-economic position can protect individuals from overall disease as well as from depressive symptoms partly through jobs that involve less material and ergonomic hazards and through the adoption of a healthier lifestyle. Particularly for depressive symptoms, education seems to offer an effective answer to childhood socio-economic disadvantage that is associated with deteriorated mental health in adult life. These findings highlight the positive association between education and individual health and ask for further research regarding the pathways that mediate this relationship, as well as regarding the policies that can secure inclusive educational contexts across countries.
The studies found have also integrated macro-level factors to a significant extent, with healthcare policy elements (i.e., care availability, out of pocket payments, gatekeeping policies, healthcare expenditure, quality of care) being the most common. Macro-economic indicators studied include gross domestic product (GDP), Gini coefficient, unemployment rates, and risk of poverty. However, social protection was less commonly used, although welfare states have been integrated in a couple of studies. These ESS studies suggest that the range of inequalities in physical and mental health between disadvantaged (i.e. women, ethnic minorities and working-class individuals) and privileged groups is subject to the national context. Some of the studies show that the availability and generousness of social protection in welfare states do not necessarily imply smaller health inequalities, even though population health is most often better in comprehensive welfare states. These findings open space for future research, which will engage with questions about the macro- level factors that reduce social inequalities in health. They also highlight that inequality “correcting” policies need to be finely tuned and targeted in order to serve their purpose.
Theoretically, the health module constituted a breaking point from the dominant research approach in the field, which focused in large part on proximate determinants of health, i.e., individual behaviors. For the first time it was possible to embed measures of health behaviors within the so- called ‘upstream’ factors of importance for cross-national variation in the patterning of health inequalities (40,44–46) and to test more recent theories such as the Fundamental Cause theory and the Institutional theory (47,51). These promising theoretical approaches would highly benefit from being tested with repeated cross-sectional data.
Studies using the Health module have been able to identify policies and interventions with the potential of reducing health inequalities. These findings have informed the policy discussion as in the case of 29 recommendations to combat social inequalities in health to the Norwegian Council on Social Inequalities in Health (59) and through several high-level meetings with European Commissioner of Health and Food Safety and high representatives from the Directorate General of Employment, Social Affairs and Inclusion. Our ESS research was also used in WHO Europe’s Health Equity Status Report initiative (60).
The success of the first Health Module demonstrates that items introduced in the first round have been found relevant both to the research and policymaking community. Therefore, we expect that most of these items will be repeated. We have carried out a systematic mapping of the use of Health Module items across the 80 publications identified in our review in order to take evidence- based decisions, in collaboration with the ESS Team and national coordinators, concerning items that could be excluded in the second round. First, an important finding emerging from our review is that all Health Module items, both health outcomes (Table 1) and social determinants (Table 2), have been examined in peer-reviewed publications. The most used social determinants continue to be behavioral determinants reflecting to some extent the predominant approach preceding the ESS Health Module in explaining health and health inequalities. Nevertheless, the impact of the ESS Health Module is visible especially in the widespread utilization of childhood and health care access determinants. In light of (i) these findings, (ii) the input of the QDT, (iii) SAB, (iv) national coordinators, and (v) the potential increased relevance of some currently less used items due to the COVID-19 crisis, we will consider the exclusion of a few items to allow for the potential inclusion of the new items presented below. In addition, a pilot testing of carefully selected (old and new) items would determine the extent to which changes to the original module are feasible.
Table 1: Health outcomes examined in
ESS Health module publications
Table 2: Social determinants examined in ESS health
module publications
| Health Outcomes
Depression |
Publications 26 |
| (Multi)morbidity | 13 |
| Self-reported health | 12 |
| Obesity | 10 |
| Limiting long-lasting illness | 7 |
| Heart conditions | 7 |
| High blood pressure | 7 |
| Cancer (past and present) | 6 |
| Diabetes | 6 |
| Pain back | 7 |
| Pain arm | 7 |
| Pain foot | 7 |
| Allergies | 5 |
| Skin conditions | 4 |
| Breathing problems | 4 |
| Stomach and digestion | 4 |
|
Severe headaches 4
Quality of housing 5
Simple concept name: Trust in healthcare system
Describe the concept in detail, outlining the various sub concepts it comprises
Many of the challenges facing Europe are the same as in other world regions, although the scale and nature may be different. This includes the continued rise of non-communicable diseases and health system pressures relating to financing and sustainability. Additionally, global surveys suggest that Europeans are the most skeptical when it comes to their trust in vaccinations, and we see growing distrust regarding the pronouncements of scientific and medical experts (61). This is a worrying direction, potentially hindering further health gains.
This distrust manifest itself in a myriad of ways, some of which include the weakening of relationships between patients and their healthcare professionals, concerns around the commodification of healthcare, the growing spread of mis- and disinformation via fake or poor- quality websites and social media communities, and active spoiler groups such as the anti-vaxx movement (62,63). This trend is of concern to policy-makers and the health community at large who are often at a loss over what to do when the facts are no longer taken as such. It is our aim, therefore, in proposing questions and gathering appropriate data within the context of the ESS, to better understand this growing distrust as affects the health arena.
There are already many studies on people’s trust in their healthcare providers (relatively well understood but poorly measured in Europe), but not to their trust in healthcare system (this is less understood, not measured, and directly relevant to those in charge of governing the system). The ESS Core and Health Module offer the possibility to ask questions about trust and health(care) in combination with people’s consideration about their role in society more generally, the conditions in which they live, access to the healthcare system, their social background, the obligations they feel their institutions and governments have towards them, and how they see themselves in the world. Examining trust in healthcare institutions in relation to these items may offer a more nuanced understanding, which will be of interest to policymakers more generally and not just the health community. In turn, this may allow for the development of policy responses at a level and in a manner of direct relevance to citizens.
Trust is a multi-dimensional concept, including not only issues that relate to the patient-doctor relationship – which are more commonly studied – but also issues that relate to public trust in health
care system. Public trust in a health care system has been defined as “an individual’s self-‐rated
degree of confidence that he or she will be adequately treated when requiring health care” (64). In
fact, trust in the healthcare system provides the contextual background in which patient–provider relationships are embedded. Researchers have argued that public trust is a better indicator of a country’s healthcare system performance than patients’ healthcare encounter experiences, because trust reflects better the perceptions of a system’s value to all citizens, not just individuals who have recently received care (65).
People’s trust in the healthcare system plays a role in explaining one’s access to and utilization of medical care, continuity of care, and even self-reported health status (66–68). Although trust in healthcare has been extensively examined in the past decades, most of the evidence comes from the United States (22) and on measures of patient-provider relations, with only one comparative study, to our knowledge, examining trust in healthcare in three European countries (21). Generally, European studies tend to be single case studies using diverse battery of questions undermining comparison between countries(69,70).
A recent systematic review identified 45 measures of trust in the health sector of which 12 measured trust in healthcare system using scales ranging from 7-59 items. The scale developed by Rose and colleagues (71) and later revised by Armstrong and colleagues (72) is a good instrument, which reflects the widely accepted understanding of trust as composed of two primary domains – a domain related to technical competence and a domain related to values congruence. Their scale has a
| Expected relationship with other complex and simple concepts
We expect trust in healthcare system to be associated with socioeconomic position, poor self-rated health, non-communicable diseases such as depression, use of healthcare, and perception of the state of healthcare from the core module (72,74). |
|
| Question wording taken from Armstrong et al. 2006: | |
| Full scale | |
| 1. The health care system does its best to make patients’ health better.* | Competence |
| 2. The health care system covers up its mistakes. | Value |
| 3. Patients receive high-quality medical care from the health care system.* | Competence |
| 4. The health care system makes too many mistakes. | Competence |
| 5. The health care system puts saving money above patients’ needs. | Value |
| 6. The health care system gives excellent medical care.* | Competence |
| 7. Patients get the same medical treatment from the health care system, no matter what the patient’s race, education or ethnicity.* |
Value |
| 8. The health care system lies to save money. | Value |
| 9. The health care system experiments on patients without them knowing. | Value |
|
Question wording taken from LaVest et al. 2009: |
|
| Full scale | |
| 1. You’d better be cautious when dealing with health care organizations | |
| 2. Patients have sometimes been deceived or misled by health care organizations | |
| 3. When health care organizations make mistakes they usually cover it up | |
| 4. Health care organizations have sometimes done harmful experiments on patients without their knowledge | |
| 5. Health care organizations don’t always keep your information totally private | |
| 6. Sometimes I wonder if health care organizations really know what they are doing | |
Simple concept name: Stress resistance
Describe the first sub concept in detail outlining any further sub concepts or specifying that it can be measured directly
The psychosocial explanation of heath inequalities has been one of the most widely researched explanations in the last two decades. This explanation posits that individual socio-psychosocial resources mediate the relationship between health and social position. Nevertheless, previous research on psychosocial mechanisms has focused largely on relative deprivation and social comparisons, rather than on how people deal with stress and adversity. Relative deprivation and social comparisons have been brought forward as important mechanisms for remaining inequalities in health in affluent societies (75). However, an earlier study based on the ESS showed that social comparisons based on income do not play a role in linking relative income to health outcomes, suggesting that social comparisons are of limited importance in explaining health inequalities (76).
According to several scholars, a psychosocial explanation of health should be considered only when social and psychological resources are examined in tandem (77–79). In order to allow for a more thorough testing of the psychosocial explanation, the ESS Health Module would benefit from complementing already existing social resources items such as social support and network with new items measuring psychological resources. In general resources, whether economic or social, do not automatically transform into a good life or a good health – resources have to be used, and they can be used more or less efficiently. Amartya Sen (80) (81) has touched on this when differing between ‘functionings’ and ‘capabilities,’ where the latter refer to the possibilities to achieve the conditions one desires. However, while Sen is mainly concerned with external obstacles to achieve the life one strives for, such as lack of personal freedom or arenas where to use one’s resources, here the focus will be on the capabilities that affect the way resources are used. Differences in health between individuals and groups will depend on the amount of resources at their disposal, but even at a given level of resources, differences in health are likely to be found. These differences will in turn depend on the way people perceive, interpret, and react to everyday hassles and demands. Hence, a concept that captures these internal processes will help us to better understand how economic and social conditions are transformed into poor health.
The concept of stress resistance generally refers to positive adaptation in the context of risk or adversity. As such, the concept is related to the concept of resilience, which has increasingly been examined at the individual level in relation to health since the financial crisis (82–84). Especially in times of sudden shocks or rapid societal change (such as the developments caused by COVID- 19), people’s ability to deal with adversity will influence the extent to which they are able to use the resources they have at their disposal. As resistance to stress under adversity is possible by developing the capacity to cope, adapt or transform hardships through absorptive, reactive, preventative and proactive measures (85) it enhances also the capacity to withstand various chronic health conditions (86).
Several complex scales ranging from 25-45 items have been designed (87,88) to measure stress and resilience, however they have been developed for use in clinical settings rather than for population health studies. As a result, public health researchers have often opted for indicators of socioeconomic position as proxies of assumed stress resistance or resilience (‘if people have high incomes, they have the resources to be stress resistant’) instead of these scales. In order to overcome this research gap, we propose to measure stress resistance more directly through a single survey item, which was first introduced in ESS Round 6. Repeating this measure in ESS Round 11 has the advantage of balancing the representation of psychosocial determinants while
| using a well-tested ESS survey item. |
| Expected relationship with other sub concepts
We expect stress resistance to be negatively related to self-reported conditions that are associated with stress, such as depressive symptoms, severe headaches, and heart problems. Also, we expect that stress resistance is influenced by people’s socioeconomic position, where people with higher education, occupational status and income, stronger social ties, and better working and housing conditions have more resources to deal with adversity. Moreover, following Sen’s arguments described above, we expect stress resistance to moderate relationships between resources and health outcomes: people are better able to fully use their resources to improve their health if they are better able to deal with adversity. |
| Question item wording
How difficult or easy do you find it to deal with important problems that come up in your life?
Extremely Extremely (Don’t difficult easy Know)
00 01 02 03 04 05 06 07 08 09 10 88 |
How the repeated module can be designed and analyzed in light of the COVID-19 crisis
Four strategies will be applied in designing and analyzing the repeated module to address the social, economic, behavioral, and health-related consequences of the COVID-19 virus, including the containment policies (i.e. lockdown) and support measures put in place to mitigate the spread and impact of the virus.
Although at varying degrees, the COVID-19 crisis has impacted social practices such as healthcare seeking and needs, health-related behaviors, the working environment, and social interactions of entire societies. Therefore, our first strategy is to track trends, by repeating items from the first module that we consider particularly sensitive to the crisis. Most of these factors have been measured in the first module such as health measures, health-related behaviors (for example alcohol consumption, physical activity etc.), health care utilization, and working conditions (job control). The successful implementation of the first Health Module has provided the basis of a perfect natural experiment that we will be able to track via a second module. The questions that we consider to be of less relevance in this respect will be candidates for exclusion (see table2) , but we will decide which ones to exclude (weighted against the benefit of adding others) during academic discussions in London with the ESS team and also based on feedback from the SAB and national coordinators.
The second strategy will be to identify essential workers during COVID-19 crisis such as health care workers (using ISCO codes), to identify the impact the crisis had on them.
The third strategy will be to explore the syndemic of COVID-19, existing non-communicable diseases (NCDs) and inequalities in the social determinants of health via the new ESS Health Module data.
Our final strategy is to evaluate the institutional effects of the crisis. We will therefore establish a contextual database (to be integrated into the existing ESS contextual data warehouse), in which we will provide scores to countries according to their responses (type, timing, duration,
consequences of violation, etc) based on various sources that have tracked government containment responses(89). The same can be done for government support measures. This, in turn, may also provide a basis for country clusters that are based on countries` responsiveness.
Team expertise and experience
The co-applicants of this proposal derive from the fields of political science, sociology, medicine, and health policy and have already published dozens of articles in high-ranked journals using both the two available health variables in the ESS core questionnaire and the ESS Health Module from 2014. All co-applicants have been involved in the design of the first module and\or used the ESS health module data extensively in their research. Most of the research employing ESS data was developed as part of the widely successful project funded by NORFACE on `Health Inequalities in European Welfare States` (HiNEWS). As part of this project over 20 articles were published with ESS Health Module data. This team has thus many years of collaborating experience.
Terje A. Eikemo holds a PhD in sociology. He is a Professor at the Dept. of Sociology and Political Science at the Norwegian University of Science and Technology (NTNU) and the leader of CHAIN. CHAIN`s mandate is to monitor, explain and reduce social inequalities globally and the ESS has been a key resource for the center. Eikemo was the principal applicant of the first ESS Health Module. He has led several international projects on health inequalities, including the European commission sponsored EURO-GBD-SE project, which collected and harmonized mortality and survey data from the early 2000s in 25 European countries in order to estimate the potential for reduction of health inequalities in Europe. Eikemo is among the most frequent users of the ESS. In 2017, Technopolis conducted a major impact study of the survey, in which Eikemo`s work on health inequalities was identified as one of four especially notable impacts of the ESS (https://www.europeansocialsurvey.org/findings/impact).
Clare Bambra holds a PhD in comparative social policy. She is Professor of Public Health, at the Institute of Population Health Sciences at the Faculty of Medical Sciences, Newcastle University, UK. She is an interdisciplinary social scientist with expertise across health politics & policy, health geography and social epidemiology. Her mixed methods research examines the social, political and economic determinants of health inequalities in Europe. She has published extensively with over 200 publications on health inequalities and has a strong international reputation in the field and a H-index of 61. She is an elected Fellow of the UK Academy of Social Sciences. She is a highly experienced researcher with several national and international leadership roles in public health: She is currently the Health Inequalities Theme lead for the NIHR School for Public Health Research and the Health Inequalities lead nationally for the ARCs (NIHR Applied Research Collaborations). She is also a Senior Investigator in the Norwegian Research Council funded CHAIN: Centre for Global Health Inequalities Research; Fuse: Centre for Translational Research in Public Health (UKCRC funded from 2008-2018); NIHR Policy Research Unit in Behavioural Science, SIPHER: UKPRP consortium on Systems Science in Public Health, and the NIHR Applied Research Collaboration – North East and North Cumbria (NE-NC-ARC). She was the Project Lead of HiNEWS. She also has experience of conducting cross-national research using national data sets including the Swedish Survey of Living Conditions and the Health Survey of England, as well as other EU-wide databases such as the European Survey of Working Conditions. She holds various advisory roles including as a member of the World Health Organisation Europe’s scientific advisory group on health equity.
Tim Huijts is research leader at the Research Centre for Education and the Labour Market (ROA), Maastricht University, The Netherlands. He obtained a PhD (cum laude) from Radboud University Nijmegen for a thesis on social inequalities in health from a cross-national perspective. He has extensive experience in cross-national comparative health research, especially using the ESS data. To date, this has resulted in over 20 international publications with the ESS data. He has
published several ESS articles with co-applicants Terje Andreas Eikemo, Clare Bambra and Mirza Balaj and is currently preparing several new joint articles. He was one of the work package leads in the HiNEWS project, and co-hosted a conference on ‘Comparing Health Across Societies’. He was also involved in the European commission sponsored EURO-GBD-SE project, which was coordinated by Terje Andreas Eikemo. In 2017 he was awarded a Philip Leverhulme Prize for outstanding research achievement.
Mirza Balaj holds a PhD in Sociology. Her thesis employed exclusively ESS data to test the Nordic paradox by developing new theoretical lens inspired by Bourdieu. Her research has been deemed cutting edge and pushing the boundaries of established knowledge in sociology of health and her research is being published in leading journals such as Sociology of Health and Illness and Social Theory and Health. Achieving such levels of innovation was only possible by comprehensive data on health and social determinants of health available by the Health Module. She has also coordinated a special issue to the European Public Health Journal on the topic of health inequalities in Europe using the ESS Health Module. Since 2016 she has published 10 articles using the Health Module. Together with Eikemo and Huijts she was also one of the authors of the ESS Toplines on Social Inequalities in Health and their Determinants. Balaj is currently the Research Coordinator of Centre for Global Health Inequalities Research CHAIN.
Kristian Heggebø holds a PhD in Social Policy. His research interests comprise socioeconomic inequalities in health, labor market analyses, and educational attainment. Moreover, he has used the ESS Round 8 recently to examine the interrelationship between climate change attitudes and social policy preferences. Cross-national comparative perspectives are cornerstone in most of his empirical work. Heggebø is familiar with both experimental, survey, and administrative register data sources, and he has published in journals such as European Sociological Review, Social Science & Medicine, European Societies, and European Journal of Social Work. Heggebø is highly skilled in statistical modeling and is e.g., responsible for the statistical training of PhD Fellows at Oslo Metropolitan University (OsloMet). Heggebø is employed as a Senior Researcher at NOVA/OsloMet and holds a postdoc position at the Centre for Global Health Inequalities Research (CHAIN).
Dissemination
Our academic and non-academic dissemination activities will be based on, and further expand on, our past successes with the first Health Module. Since the implementation of our module from 2014, we have established CHAIN (https://www.ntnu.edu/chain), a global centre for the international study of health inequalities (supported by a NOK 100 Million budget), which has its own dissemination division. This work is guided by EuroHealthNet (EHN), a large non-profit partnership organisation based in Brussels, which works to improve and sustain health in European countries through action on the social determinants of health. EHN`s policy platform helps us monitor and influence European policy relating to health equity, particularly towards the European Commission. A new Health Module will be placed in the heart of these activities. We have already extensive experience in organising and participating on high-level policy impact events. We have presented our previous ESS research to European Governments and the European Commission, including to the previous Minister for Health and Food Safety, Vytenis Andriukaitis, on two occasions. We also have strong links with WHO Europe – for example, Bambra is a member of the World Health Organisation Europe’s scientific advisory group on health equity.
Our planned dissemination of a potential new module will not be restricted to our outputs. We also plan to disseminate the longstanding process leading to the new module. By doing so, we will not only bring further attention to the upcoming module as such (which will lead to increased utilization once it becomes available), but also to the rigorous methodologies applied by ESS as an internationally leading social survey, and to the people running it.
Moreover, we will ensure knowledge transfer of the process and the results (once the Module is accessible) to ensure 1) good visibility among stakeholder groups (we have identified 3600 so far) and maximum impact in terms of research, policy and practical relevance; 2) multiplication of findings in appropriate research and policy processes; and 3) translation of research findings to a general audience (popular science).
Biannual newsletters will be sent out to our stakeholders, to EHN members and CHAIN partners (such as the WHO, UNICEF and the Bill & Melinda Gates-funded Global Burden of Disease Study). ESS updates will be regularly disseminated on CHAIN Facebook and Twitter accounts, we will provide news releases as needed, mostly to promote publications and events. We will respond to EU policy developments through consultations and by publishing infographics, policy briefs, and an ESS Topline Report (similarly to the one we prepared for the 2014 module). We will organise capacity-building events such as World Leadership Dialogues, webinars with the UNESCO Chair on Education and Health, the World Health Summit and the World Congress on Public Health. In addition to this, CHAIN will provide an annual report, including our ESS activities.
As the track of publication activities shows (see table 3), the previous module has been used extensively. We have detected 80 publications, and the number is increasing by the year. We plan to kick-off the scientific dissemination by submitting a new study design article to a suitable journal in collaboration with the ESS team. Our previous study design article published in the European Sociological Review is already among their most cited studies. Further, inspired by the success of our special issue based on the first ESS Health Module (published in the Eur J Public Health), we will aim at publishing a new special issue in a high-ranked journal. This is a very effective way to make full use of all items and provide a synthesis of their joint contribution. Next to this, we will continuously be submitting research articles to separate journals. Our research outputs will be presented at international sociological and public health conferences. We will also apply for a separate session at the first upcoming ESS conference after the release of the survey.
Table 3: ESS Health Module based publications and citations
| Number of articles identified | Number of citations |
| 80 | 1610 |
The annual report and our scientific publications will be available to scientists, national health authorities, health promotion institutes, ministries of health, policy makers, private stakeholders and the general public. We further aim to contribute to open science in accordance with Science Europe’s Principles. We will also be able to obtain visibility within the WHO, as we have been commissioned by them to provide a global equity report.
CHAIN has been extremely successful in obtaining funding for its research over the last 5 years (for example we led the Hi-NEWS Health Inequalities in European Welfare States consortium – funded by NORFACE). Our chances of obtaining new grants that can support analysis and dissemination of the repeated module, will increase as there will be high demand for research that can track trends of health and health determinants in the post COVID-19 era, still for many years to come.
We will be continuously searching for grant opportunities and we have large capacity and experience in writing competitive proposals. A new health module will provide us with a competitive advantage, both in national (Norwegian Research Council and Dutch Science Foundation) and international (for example Horizon Europe, ERC, Norface, and Nordforsk) calls. In addition to this, we expect NTNU to provide us with a PhD position as a bonus for getting the module. We would be very interested in applying for Horizon Europe grants in collaboration with the ESS.
The work on our 2014 Module started 8 years ago. As our ambition is to repeat our module on a regular basis, we have an 8-year plan for the new module (counting from the date our proposal would be accepted).
Year 0 – 2: Dissemination of the development of the module (newsletters, social media). Year 2 – 3: Submission of a study design article.
Organisation of a health inequalities session at an ESS conference. New ESS Topline Report.
Identify a suitable journal for a special issue capturing trends since 2014 in light of COVID-19.
Year 3 – 5: Work on and submit articles for a journal special issue.
Apply for national and EU-grants that are built around our two health modules.
Year 6 – 8: Work on a book (potentially Oxford University Press) based on our ESS publications till this date.
Preparation and potential submission (if we think the timing is right) of a new health module application.
All years: Regular newsletters, social media presentations, conference presentations, policy- events, capacity building events, continuously looking for funding opportunities, and joint policy and research activities with City University to promote the ESS.
CURRICULUM VITAE: TERJE ANDREAS EIKEMO
Email: Terje.Eikemo@ntnu.no Phone no: +47 99034077
EDUCATION
PhD in Sociology at NTNU (date of defence: June 6, 2008)
CURRENT POSITIONS
Leader of CHAIN – Centre for Global Health Inequalities Research: www.ntnu.edu/chain
Professor of Sociology, Dept of Sociology and Political Science (NTNU)
PROJECT MANAGEMENT EXPERIENCE / FUNDING (SELECTION)
2019 – 2024 Project leader of the Global Health Inequality Project (funded by the Norwegian Research Council, BEDREHELSE program). Total budget: NOK 93 Million. NTNU.
2017 Head of the international team behind the health module of the U.S. based General Social Survey 2016.
2017 – 2019 Member of the Scientific Advisory Board of the European Social Survey
2016 – Editor-in-Chief of the Scandinavian Journal of Public Health, 2015 – 2016 Vice President: European Society for Health and Medical
Sociology (ESHMS).
2015 – 2019 Co-leader of the HiNews project (Health inequalities in European welfare states),funded by the NORFACE Welfare state futures program. Budget: EUR 1,5 Million.
2012 – 2014 Head of the European Social Survey (ESS) Question module Design Team (QDT) on Social Inequalities in Health and their Determinants (round 7).
A SELECTION OF RELEVANT PUBLICATIONS
1 Rydland H, Solheim, E, & Eikemo, T.A. (forthcoming). Educational inequalities in high- vs. low – preventable health conditions: exploring the fundamental cause theory. Social Science & Medicine.
- Mutyambizi, , Booysen, F., Stornes, P., & Eikemo, T.A. (2019). Subjective social status and inequalities in depressive symptoms: a gender-specific decomposition analysis for South Africa. International Journal for Equity in Health, 18(1).
- Beckfield J, Balaj M, […] & Eikemo (2017). The health of European populations: introduction to the special supplement on the 2014 European Social Survey (ESS) rotating module on the social determinants of health. European Journal of Public Health. 1;27(suppl_1): 8-13.
- Eikemo, A., Huijts, T., Bambra, C,. & Fitzgerald, R. (2016). The first pan-European sociological health inequalities survey of the general population: the European Social Survey (ESS) rotating module on the social determinants of health. European Sociological Review, doi: 10.1093/esr/jcw019
- Beckfield, , Bambra, C., Eikemo, T.A., Hujits, T., McNamara, C., & Wendt, C. (2015). Towards an institutional theory of welfare state effects on the distribution of population health. Social Theory & Health, 13, 227–244. doi:10.1057/sth.2015.192014
- Van de Velde, , Bambra, C., Eikemo, T. A., Bracke, P. Keeping it in the family: the self-rated health of lone mothers in different European welfare regimes. (2014). Sociology of Health & Illness, 36(8):1220-42. doi: 10.1111/1467-9566.12162.
- Eikemo, A., Bambra, C., Judge, K., & Ringdal, K. (2008). Welfare state regimes and differences in self-perceived health in Europe: A multilevel analysis. Social Science & Medicine, 66(11), 2281-2295.
- Eikemo, A., Huisman, M., Bambra, C., & Kunst, A. E. (2008). Health inequalities according to educational level in different welfare regimes: a comparison of 23 European countries. Sociology of Health & Illness, 30(4), 565-582.
CURRICULUM VITAE: PROFESSOR CLARE BAMBRA
EDUCATIONAL QUALIFICATIONS
2002 PhD, Department of Government, University of Manchester
1999 MA Econ, European Politics and Policy, University of Manchester, with Distinction 1998 BSoc Sc, Political Science, University of Birmingham, 1st class (hons) EMPLOYMENT HISTORY
2017 – date Professor of Public Health, Population Health Sciences Institute, Newcastle University
2005 – 2016 Lecturer/Reader/Professor, Department of Geography, Durham University
2004 – 2005 Lecturer, Social Research, Department of Sociology, Sheffield Hallam University 2002 – 2004 Research associate, Department of Public Health, University of Liverpool CURRENT GRANTS
NIHR Applied Research Collaboration – North East and North Cumbria (NE-NC-ARC), £9 million, 2019-2024 NIHR
System-science Informed Public Health and Economic Research for Non-communicable Disease Prevention (the SIPHER Consortium), UK Prevention Research Partnership, £4.98 million
Centre for Global Health Inequalities Research, Norwegian Research Council, €7 million 2019- 2024
Policy Research Unit Behavioural Science, £4.8 million NIHR.
Communities in Control Study: An evaluation of a natural policy experiment in community empowerment – phase 3. NIHR Public Health Research Panel, £659,000, 2018-2022
NIHR School of Public Health 2. Department of Health and NIHR, 2017-2022, £1,800,000.
PREVIOUS RESEARCH GRANTS (SELECTION)
PI: Local health inequalities in an age of austerity: the Stockton on Tees study. Leverhulme Trust Research Leadership Grant, 2013-2018, £997,000.
PI: Health Inequalities and Economic Productivity, Northern Health Sciences Alliance, 2018,
£45,000.
PI: HiNEWS Consortium: Health Inequalities in European Welfare States, Norface, 2015–2018,
€1,200,000
PI: Equal North Research and Practice network, Public Health England, 2016-2017, £60,000. PI: Tackling inequalities in obesity, NIHR National Institute for Health Research, 2011–2013,
£260,000
PI: Inequalities in the population health effects of economic recession and economic growth: a comparative multi-level study, Bupa Foundation, 2009–2013, £170,000
PI: Evaluating the Durham Worklessness Model, National Health Service, 2009–2013, £550,000 PI: Capacity Building Fellowship in Public Health Policy, National Health Service, 2005–2010,
£550,000
Co-I: Fuse: Centre for Translational Research in Public Health. MRC, 2013-2018, £3,400,000. Co-I: Recession and Mental Health in Scotland: Do Personal or Community Factors promote
Resilience to Labour Market Change? ESRC £161,000, 2018-19
Co-I: Community pHarmaciEs Mood Intervention STudy (CHEMIST): Feasibility and Pilot Study, NIHR, 2018-2020, £467,000
| Total Publications | Total Citations | h–index | i10–index |
| 210 | 13,144 | 61 | 144 |
| Source: Google Scholar (May 2020) | |||
CURRICULUM VITAE: TIM HUIJTS
Dr. Tim Huijts is research leader at the Research Centre for Education and the Labour Market (ROA), Maastricht University, the Netherlands. He obtained an MSc (2006, cum laude) and PhD (2011, cum laude) in Sociology at the Radboud University Nijmegen. Before joining Maastricht University in April 2018 he worked as Assistant Professor at Utrecht University, Postdoctoral Researcher at the University of Oxford, Lecturer at Queen Mary University of London, and Senior Lecturer at the University of York. In his research he examines how national and institutional factors influence social inequalities, and how these factors moderate the impact of education and employment on outcomes such as health and well-being. He has co-authored over 50 international peer-reviewed journal publications, and his work has appeared in a broad range of journals in Sociology, Demography and Public Health. He was a co-applicant for the NORFACE-funded (1.1 million euros) HiNEWS project (2015-2018), which examined why social inequalities persist in European welfare states and what can be done to reduce them. Additionally, together with international colleagues he developed the rotating module on ‘Social inequalities in health and their determinants’ for the 7th round of the European Social Survey (2014). His research was recognized with a Philip Leverhulme Prize (2017) for outstanding achievement.
Key publications:
Gkiouleka, A., Huijts, T., Beckfield, J. & Bambra, C. (2018). Understanding the micro and macro politics of health: inequalities, intersectionality & institutions – a research agenda. Social Science & Medicine, 200, 92-98.
Huijts, T., Gkiouleka, A., Reibling, N., Thomson, K., Eikemo, T. & Bambra, C. (2017). Educational inequalities in risky health behaviours in 21 European countries: Findings from the European social survey (2014) special module on the social determinants of health. European Journal of Public Health, 27, 63-72.
Blom, N., Huijts, T., & Kraaykamp, G. (2016). Ethnic health inequalities in Europe. The moderating and amplifying role of healthcare system characteristics. Social Science & Medicine, 158, 43-51.
Van de Velde, S., Huijts, T., Bambra, C., & Bracke, P. (2013). Macro-level gender equality and depression in men and women in Europe. Sociology of Health and Illness, 35, 682-698.
Huijts, T. & Kraaykamp, G. (2012). Immigrants’ health in Europe: a cross-classified multilevel approach to examine origin country, destination country, and community effects. International Migration Review, 46, 101-137.
Huijts, T., Eikemo, T.A. & Skalicka, V. (2010). Income-related health inequalities in the Nordic countries: examining the role of education, occupational class, and age. Social Science & Medicine, 71, 1964-1972.
Subramanian, S.V., Huijts, T. & Avendano, M. (2010). Self-reported health assessments in the 2002 World Health Survey: how do they correlate with education? Bulletin of the World Health Organization, 88, 131-138.
CURRICULUM VITAE: MIRZA BALAJ
Address: Department for Sociology and Political Science Faculty of Social and Educational Science
Norwegian University of Science and Technology (NTNU) Email: mirza.balaj@ntnu.no
Phone no: +4794296342
CURRENT POSITION:
Postdoc, Department for Sociology and Political Science, NTNU Research Coordinator, Center for Global Health Inequalities Research
EDUCATION
2015 – 2018 PhD Fellow in Sociology, Department for Sociology and Political Science, NTNU 2011 – 2013 MSc, European Politics and Policies, University of Leuven, with Magna Cum Laude
PROJECT EXPERIENCE
2019 – ongoing Coordinator of Global Health Inequality Project. Funded by the Norwegian Research Council for a total budget of NOK 93 Million.
2016 – 2018 Member of the HEALTHDOX project (The Paradox of Health State Futures). 2015 – 2017 Member of the HiNEWS project (Health Inequalities in European Welfare States)
PUBLICATIONS (selected):
Balaj M, Huijts T, McNamara CL, Bambra C, Eikemo TA. Non-communicable diseases and the social determinants of health in the Nordic countries: Findings from the European Social Survey (2014) special module on the social determinants of health, SJPH, 2017, doi: 10.1177/1403494816686026
Balaj M, McNamara C.L, Eikemo T.A, Bambra C. The social determinants of inequalities in self- reported health in Europe: findings from the European social survey (2014) special module on the social determinants of health. Eur J Public Health 2017;27:107–114.
Beckfield J, Balaj M, McNamara C.L, Huijts T, Bambra C, Eikemo TA. The health of European populations: introduction to the special supplement on the 2014 European Social Survey (ESS) rotating module on the social determinants of health. . Eur J Public Health 2017;27: 3-7
McNamara C.L, Balaj M, Thomson HK, et al. The socioeconomic distribution of non-communicable diseases in Europe: findings from the European social survey (2014) special module on the social determinants of health. Eur J Public Health 2017;27:22–26.
Bøe T, Balaj M, Eikemo TA, et al. Financial Difficulties in Childhood and Adult Depression in Europe: findings from the European social survey (2014) special module on the social determinants of health. Eur J Public Health 2017;27:96–101.
Balaj M, Eikemo, T.A. Sick of social status: A Bourdieusian perspective on morbidity and health. Sociology of Health and Illness. (forthcoming)
Balaj M. Self-reported health and the social body. Social Theory & Health. (forthcoming)
Balaj M. Albania Health Policies and Politics .in Ellen Immergut (eds.) Health Politics in Europe: A Handbook. Oxford University Press (forthcoming)
CURRICULUM VITAE: KRISTIAN HEGGEBØ
Born: 18.12.1988, Haugesund; Citizenship: Norwegian
E-mail: kristian.heggebo@oslomet.no and kristian.heggebo@gmail.com
Current position:
Senior researcher, NOVA, OsloMet – Oslo Metropolitan University
Postdoc, CHAIN, NTNU – Norwegian University of Science and Technology
Work experience:
2016— Researcher/ Senior researcher, NOVA, OsloMet – Oslo Metropolitan University 2013—2016 PhD fellow, Faculty of Social Sciences, Oslo and Akershus University College of
Applied Sciences
Academic Degrees:
2016: PhD in social work and social policy. Dissertation title: “Hiring, Firing, and Health – A Cross-National Comparative Perspective”, Oslo and Akershus University College
2012: Master’s degree, sociology, University of Oslo
Publications (selected):
-Heggebø, K., van der Wel, K. A, & Dahl, E. (2019). Does social capital matter more when health status is poor? Labor market attachment among long-term recipients of social assistance in Norway. Published online 19 November, European Journal of Social Work.
-Heggebø, K. & Buffel, V. (2019). Is there less labor market exclusion of people with ill health in flexicurity’ countries? Comparative evidence from Denmark, Norway, the Netherlands, and Belgium. International Journal of Health Services 49(3): 476-515.
-Heggebø, K; Tøge, A. G.; Dahl, E. & Berg, J. E. (2019). Socioeconomic inequalities in health during the Great Recession: A scoping review of the research literature. Scandinavian Journal of Public Health, 47(6): 635–654.
-Heggebø, K. & Elstad, J. I. (2018). Is it easier to be unemployed when the experience is more widely shared? Effects of unemployment on self-rated health in 25 European countries with diverging macroeconomic conditions. European Sociological Review, 34(1): 22-39.
-Heggebø, K. (2017). Are immigrants and descendants with ill health more prone to unemployment? Evidence from 18 European countries. Ethnicity & Health, 22(4): 402-424.
-Birkelund, G. E.; Heggebø, K.; & Rogstad, J. (2017). Additive or multiplicative disadvantage? The scarring effects of unemployment for ethnic minorities. European Sociological Review, 33(1): 17- 29.
-Heggebø, K. (2016). Health effects of unemployment in Denmark, Norway and Sweden 2007– 2010: Differing economic conditions, differing results? International Journal of Health Services, 46(3): 406-
-Heggebø, K. & Dahl, E. (2015). Unemployment and health in diverging economic conditions: Compositional changes? Evidence from 28 European countries. International Journal for Equity in Health, 14: 121.
Submitted and working papers (selected):
Heggebø, K., Dahl, E & van der Wel, K. A. “Disentangling the dynamics of social assistance: A linked survey—register data cohort study of long-term social assistance recipients in Norway”.
Heggebø, K.; Jakobsson, N.; Muttarak, R.; Schøyen, M. A. “Climate change attitudes in Europe – Does the prevailing economic conditions matter?”
Heggebø, K. & Elstad, J. I. “Anatomy of the Norwegian income and wealth distribution 2000— 2015: Do immigrants fare worse when the immigrant population grows?”
References
- Chowdhury R, Heng K, Shawon MSR, Goh G, Okonofua D, Ochoa-Rosales C, et Dynamic interventions to control COVID-19 pandemic: a multivariate prediction modelling study comparing 16 worldwide countries. European journal of epidemiology. 2020;35(5):389–99.
- European Coronavirus Response Using every available euro in every way possible to protect lives and livelihoods [Internet]. COM/2020/143; 2020. Available from: https://eur-lex.europa.eu/legal- content/EN/TXT/?uri=CELEX%3A52020DC0143
- European Communication-The EU budget powering the recovery plan for Europe. 2020.
- Publishing. In it together: Why less inequality benefits all. OECD publishing; 2015.
- Morris J, Donkin A, Wonderling D, Wilkinson P, Dowler A minimum income for healthy living. Journal of Epidemiology & Community Health. 2000;54(12):885–9.
- Lynch JW, Kaplan GA, Salonen Why do poor people behave poorly? Variation in adult health behaviours and psychosocial characteristics by stages of the socioeconomic lifecourse. Social science & medicine. 1997;44(6):809–19.
- International Labour Office (ILO). Non-‐standard employment around the world: Understanding challenges, shaping
prospects. 2016;
- Rodgers G, Rodgers Precarious jobs in labour market regulation: The growth of atypical employment in Western Europe. International Labour Organisation; 1989.
- Kalleberg Precarious work, insecure workers: Employment relations in transition. American sociological review. 2009;74(1):1–22.
- Population by educational attainment level, sex and age (%). Population by educational attainment level, sex and age (%). [Internet]. 2020 [cited 2020 Jan 17]. Available from: https://appsso.eurostat.ec.europa.eu/nui/show.do?dataset=edat_lfs_9903&lang=en
- Heisig JP, Gesthuizen M, Solga Lack of skills or formal qualifications? New evidence on cross-country differences in the labor market disadvantage of less-educated adults. Social science research. 2019;83:102314.
- Bäckman O, Jakobsen V, Lorentzen T, Österbacka E, Dahl Early school leaving in Scandinavia: Extent and labour market effects. Journal of European Social Policy. 2015;25(3):253–69.
- Bambra C, Eikemo Welfare state regimes, unemployment and health: a comparative study of the relationship between unemployment and self-reported health in 23 European countries. Journal of Epidemiology & Community Health. 2009;63(2):92–8.
- Mortensen MB, Falk E, Schmidt Twenty-year nationwide trends in statin utilization and expenditure in Denmark. Circulation: Cardiovascular Quality and Outcomes. 2017;10(7):e003811.
- WHO Regional Office for The European health report 2018. More than numbers – evidence for all. Highlights. [Internet]. WHO; 2018. Available from:
https://www.euro.who.int/ data/assets/pdf_file/0003/380478/HEALTH_REPORT_HIGHLIGHTS_2018_EN.PDF
- Wilkins E, Wilson L, Wickramasinghe K, Bhatnagar P, Leal J, Luengo-Fernandez R, et European cardiovascular disease statistics 2017. 2017;
- WHO-GHO. Raised blood pressure , age-standardized (%) Estimates by country [Internet]. Available from: https://apps.who.int/gho/data/node.main.A875STANDARD?lang=en
- Non-Medical Determinants of Health [Internet]. 2020. Available from: https://stats.oecd.org/viewhtml.aspx?datasetcode=HEALTH_LVNG&hx0026;lang=en;#
- Timmis A, Townsend N, Gale CP, Torbica A, Lettino M, Petersen SE, et European Society of Cardiology: cardiovascular disease statistics 2019. European Heart Journal. 2020;41(1):12–85.
- Bieber Global Nationalism in Times of the COVID Pandemic. Nationalities Papers. 2020;1–19.
- van Der Schee E, Braun B, Calnan M, Schnee M, Groenewegen Public trust in health care: a comparison of Germany, the Netherlands, and England and Wales. Health Policy. 2007;81(1):56–67.
- Ozawa S, Sripad How do you measure trust in the health system? A systematic review of the literature. Social Science & Medicine. 2013;91:10–4.
- Employment rates by sex, age and citizenship (%) [Internet]. 2020. Available from: https://appsso.eurostat.ec.europa.eu/nui/show.do?dataset=lfsa_ergan&lang=en
- The COVID-19 response: Getting gender equality right for a better future for women at work [Internet]. 2020. Available from: https://www.ilo.org/wcmsp5/groups/public/—dgreports/— gender/documents/publication/wcms_744374.pdf
- Mackenbach JP, Bopp M, Deboosere P, Kovacs K, Leinsalu M, Martikainen P, et Determinants of the magnitude of socioeconomic inequalities in mortality: A study of 17 European countries. Health & Place. 2017 Sep 1;47:44–53.
- McNamara CL, Balaj M, Thomson KH, Eikemo TA, Solheim EF, Bambra The socioeconomic distribution of non- communicable diseases in Europe: findings from the European Social Survey (2014) special module on the social determinants of health. The European Journal of Public Health. 2017;27(suppl_1):22–6.
- Beckfield J, Bambra C, Eikemo TA, Huijts T, McNamara C, Wendt An institutional theory of welfare state effects on the distribution of population health. Soc Theory Health. 2015 Aug 1;13(3):227–44.
- Busemeyer MR, de la Porte C, Garritzmann JL, Pavolini The future of the social investment state: politics, policies, and outcomes. Journal of European public policy. 2018;25(6):801–9.
- von der Leyen Opening Statement in the European Parliament Plenary Session by Ursula von der Leyen, Candidate for President of the European Commission [Internet]. 2019. Available from: https://ec.europa.eu/commission/presscorner/detail/en/SPEECH_19_4230
- Bambra C, Riordan R, Ford J, Matthews The COVID-19 Pandemic and Health Inequalities. Journal of Epidemiology and Community Health. 2020;
- Dahlgren G, Whitehead Policies and strategies to promote social equity in health. 1991;
- Marmot M, Wilkinson Social determinants of health. OUP Oxford; 2005.
- Marmot M, Allen J, Goldblatt P, Boyce T, McNeish D, Grady M, et The Marmot review: Fair society, healthy lives. London: UCL. 2010;
- Lundberg O, Lahelma Nordic health inequalities in the European context. Nordic welfare states in the European context. 2001;42–65.
- Bartley Health inequality: an introduction to concepts, theories and methods. John Wiley & Sons; 2016.
- Joyce K, Bambra Health inequalities in developed nations. Social Alternatives. 2010;29(2):21–7.
- Cockerham WC, Hamby BW, Oates The social determinants of chronic disease. 2017;
- Skalická V, Van Lenthe F, Bambra C, Krokstad S, Mackenbach Material, psychosocial, behavioural and biomedical factors in the explanation of relative socio-economic inequalities in mortality: evidence from the HUNT study. International journal of epidemiology. 2009;38(5):1272–84.
- Papazoglou M, Galariotis Revisiting the Effect of Income on Health in Europe: Evidence from the 8th Round of the European Social Survey. Soc Indic Res. 2020 Feb 1;148(1):281–96.
- Balaj M, McNamara CL, Eikemo TA, Bambra The social determinants of inequalities in self-reported health in Europe: findings from the European social survey (2014) special module on the social determinants of health. European Journal of Public Health. 2017;27(suppl_1):107–14.
- Hoven H, Siegrist Work characteristics, socioeconomic position and health: a systematic review of mediation and moderation effects in prospective studies. Occup Environ Med. 2013 Sep 1;70(9):663–9.
- Phelan JC, Link BG, Tehranifar Social conditions as fundamental causes of health inequalities: theory, evidence, and policy implications. Journal of health and social behavior. 2010;51(1_suppl):S28–40.
- Link BG, Phelan Social conditions as fundamental causes of disease. Journal of health and social behavior. 1995;80–94.
- Mackenbach JP, Valverde JR, Bopp M, Brønnum-Hansen H, Deboosere P, Kalediene R, et Determinants of inequalities in life expectancy: an international comparative study of eight risk factors. The Lancet Public Health. 2019;4(10):e529–37.
- Gkiouleka A, Avrami L, Kostaki A, Huijts T, Eikemo TA, Stathopoulou Depressive symptoms among migrants and non-migrants in Europe: documenting and explaining inequalities in times of socio-economic instability. European journal of public health. 2018;28(suppl_5):54–60.
- Šmitas A, Gustainienė How do emotional, cognitive and social health resources relate to health behaviour? The case of Lithuania. Tarptautinis psichologijos žurnalas: biopsichosocialinis požiūris= International journal of psychology: a biopsychosocial approach Kaunas: Vytauto Didžiojo universitetas, 2017, Nr 21. 2017;
- Rydland Educational inequalities in high- vs. low – preventable health conditions: exploring the fundamental cause theory. Social Science & Medicine. (forthcoming);
- Schrecker T, Bambra How politics makes us sick: Neoliberal epidemics. Springer; 2015.
- Beckfield J, Bambra Shorter lives in stingier states: Social policy shortcomings help explain the US mortality disadvantage. Social Science & Medicine. 2016;171:30–8.
- Gkiouleka A, Huijts T, Beckfield J, Bambra Understanding the micro and macro politics of health: Inequalities, intersectionality & institutions-A research agenda. Social Science & Medicine. 2018;200:92–8.
- Balaj M, Eikemo Sick of social status: A Bourdieusian perspective on morbidity and health. Sociology of Health
& Illness. (forthcoming);
- Catalan Agency for Health Quality and Coronavirus SARS-Cov-2 interactive map. [Internet]. 2020 [cited 2020 Jun 15]. Available from: e http://aquas.gencat.cat/.content/IntegradorServeis/mapa_ covid/atlas.html
- Chen J, Krieger Revealing the unequal burden of COVID-19 by income, race/ethnicity, and household crowding: US county vs. ZIP code analyses. Harvard Center for Population and Development Studies Working Paper Series. 2020;19(1).
- Office for National Deaths involving COVID-19 by local area and socioeconomic deprivation: deaths occurring between 1 March and 31 May 2020 [Internet]. 2020. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsinvolvin gcovid19bylocalareasanddeprivation/deathsoccurringbetween1marchand31may2020
- Segerstrom SC, Miller Psychological stress and the human immune system: a meta-analytic study of 30 years of inquiry. Psychological bulletin. 2004;130(4):601.
- Eikemo TA, Bambra C, Huijts T, Fitzgerald The first pan-European sociological health inequalities survey of the general population: the European Social Survey rotating module on the social determinants of health. European Sociological Review. 2017;33(1):137–53.
- Malnar ESS annual bibliographic report 2018 [Internet]. 2018. Available from: http://www.europeansocialsurvey.org/docs/findings/ESS-ERIC-Deliverable-10.3-ESS-Annual-Bibliographic-Report- 2018.pdf
- Beckfield J, Balaj M, McNamara CL, Huijts T, Bambra C, Eikemo The health of European populations: introduction to the special supplement on the 2014 European Social Survey (ESS) rotating module on the social determinants of health. European Journal of Public Health. 2017;27(suppl_1):3–7.
- Arntzen A, Bøe T, Dahl E, Drange N, Eikemo TA, Elstad JI, et 29 recommendations to combat social inequalities in health. The Norwegian Council on Social Inequalities in Health. Scandinavian journal of public health. 2019;47(6):598–605.
- Bambra C, Thomson Reducing inequities in health across the life-course: Transition to independent living– Young adults. Reducing inequities in health across the life-course. 2019;
- Europe Vaccination and trust—How concerns arise and the role of communication in mitigating crises. 2017;
- Vosoughi S, Roy D, Aral The spread of true and false news online. Science. 2018;359(6380):1146–51.
- Kim Trust in health information websites: A systematic literature review on the antecedents of trust. Health informatics journal. 2016;22(2):355–69.
- Straten GF, Friele RD, Groenewegen Public trust in Dutch health care. Social science & medicine. 2002;55(2):227–34.
- Gilson Trust and the development of health care as a social institution. Social science & medicine. 2003;56(7):1453–68.
- Russell Treatment-seeking behaviour in urban Sri Lanka: trusting the state, trusting private providers. Social science & medicine. 2005;61(7):1396–407.
- Hall MA, Zheng B, Dugan E, Camacho F, Kidd KE, Mishra A, et Measuring patients’ trust in their primary care providers. Medical care research and review. 2002;59(3):293–318.
- Wang H, Schlesinger M, Wang H, Hsiao The flip-side of social capital: the distinctive influences of trust and mistrust on health in rural China. Social Science & Medicine. 2009;68(1):133–42.
- Calnan MW, Sanford Public trust in health care: the system or the doctor? BMJ Quality & Safety. 2004;13(2):92–7.
- Mohseni M, Lindstrom Social capital, trust in the health-care system and self-rated health: the role of access to health care in a population-based study. Social science & medicine. 2007;64(7):1373–83.
- Rose A, Peters N, Shea JA, Armstrong ORIGINAL ARTICLE Development and Testing of the Health Care System Distrust Scale. JGIM: Journal of General Internal Medicine. 2004;19(1).
- Armstrong K, Rose A, Peters N, Long JA, McMurphy S, Shea Distrust of the health care system and self- reported health in the United States. Journal of general internal medicine. 2006;21(4):292.
- LaVeist TA, Isaac LA, Williams Mistrust of Health Care Organizations Is Associated with Underutilization of Health Services. Health Services Research. 2009 Dec 1;44(6):2093–105.
- Musa D, Schulz R, Harris R, Silverman M, Thomas Trust in the health care system and the use of preventive health services by older black and white adults. American journal of public health. 2009;99(7):1293–9.
- Wilkinson R, Pickett The spirit level: Why equality is better for everyone. Penguin UK; 2010.
- Präg P, Mills M, Wittek Income and Income Inequality as Social Determinants of Health: Do Social Comparisons Play a Role? Eur Sociol Rev. 2014 Apr 1;30(2):218–29.
- Dagdeviren H, Donoghue M, Promberger Resilience, hardship and social conditions. Journal of Social Policy. 2016;45(1):1–20.
- Thoits Stress and health: Major findings and policy implications. Journal of health and social behavior. 2010;51(1_suppl):S41–S53.
- Whitehead M, Pennington A, Orton L, Nayak S, Petticrew M, Sowden A, et How could differences in ‘control over destiny’lead to socio-economic inequalities in health? A synthesis of theories and pathways in the living environment. Health & place. 2016;39:51–61.
- Sen K.(1985),“Commodities and Capabilities.” 1989;
- Sen Inequality explained. Cambridge, Mass: Harvard University. 1992;
- Glonti K, Gordeev VS, Goryakin Y, Reeves A, Stuckler D, McKee M, et A Systematic Review on Health Resilience to Economic Crises. PLoS One [Internet]. 2015 Apr 23 [cited 2020 Jun 16];10(4). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4408106/
- Castleden M, McKee M, Murray V, Leonardi Resilience thinking in health protection. Journal of Public Health. 2011;33(3):369–77.
- Friedli L, World Health Mental health, resilience and inequalities. Copenhagen: WHO Regional Office for Europe:; 2009.
- Keck M, Sakdapolrak What is social resilience? Lessons learned and ways forward. Erdkunde. 2013;5–19.
- Perna L, Mielck A, Lacruz ME, Emeny RT, Rothe A von E, Meisinger C, et The association between resilience and diabetic neuropathy by socioeconomic position: Cross-sectional findings from the KORA-Age study: Journal of Health Psychology [Internet]. 2013 Nov 27 [cited 2020 Jun 16]; Available from: https://journals.sagepub.com/doi/10.1177/1359105313510334
- Connor KM, Davidson Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD- RISC). Depress Anxiety. 2003;18(2):76–82.
- Friborg O, Hjemdal O, Rosenvinge JH, Martinussen A new rating scale for adult resilience: what are the central protective resources behind healthy adjustment? International Journal of Methods in Psychiatric Research. 2003;12(2):65–76.
- Hale T, Webster S, Petherick A, Phillips T, Kira Oxford covid-19 government response tracker. Blavatnik School of Government. 2020;25.


